
Treatment
After being diagnosed with SCFE, the patient should stop weight-bearing immediately and receive surgery within 24-48 hours to prevent the displaced femoral head from slipping any further.
If SCFE is diagnosed at an early stage, there is a greater chance of stabilizing the hip without complications. The specific surgical procedure that a patient receives will depend on the severity of their slip.
Following surgery, patients will require crutches and slowly return to weight-bearing based on the advice of their doctor. During this transition, a physiotherapist can also provide activities to strengthen the hip and improve flexibility. Time to return to sports and physical activities will vary depending on patient circumstances.
Typically, a patient will have follow-up doctor visits every 3-4 months for a 2-year period to ensure no complications arise. Based on the patient’s age and other clinical characteristics, it may also be necessary to follow up with a dietician or endocrinologist.
Procedures
-
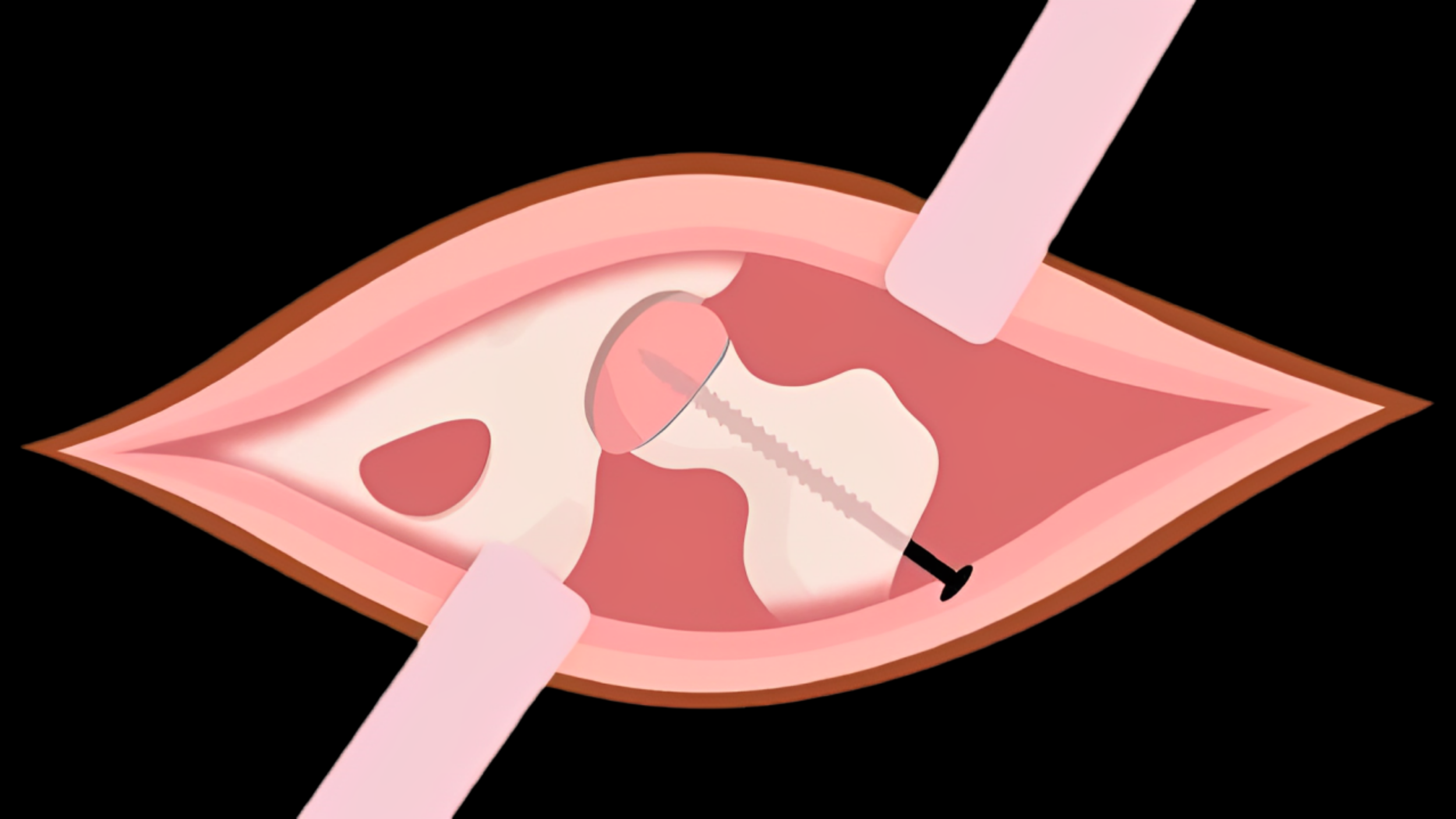
This procedure is often used for patients with stable SCFE. After making a small incision near the hip, the physician inserts a metal screw across the growth plate to prevent slippage of the femoral head and maintain an anatomic position.
Following surgery, the growth plate will gradually close over time and, once closed, the femoral head will be unable to slip.
-
Patients with unstable SCFE will typically undergo open reduction. In this procedure, the physician makes a small incision at the hip and physically manipulates, or reduces, the femoral head back to anatomic position. After reduction, the physician will insert a metal screw to maintain the position of the femur as the growth plate closes over time.
Compared with in-situ fixation, open reduction is a more extensive surgery and involves a longer recovery.
-
Patients with a SCFE on one side sometimes develop a SCFE on the other side. There are some factors that may increase the risk of a slip of the other hip including younger age, higher body mass index, disorders of the endocrine system, and x-ray findings.
Your doctor will assess your child’s risk, and if the risk is noted to be high, your doctor may recommend placing a screw in the other hip (known as “prophylactic fixation”). Even if prophylactic fixation is not performed, close follow-up and periodic x-rays are needed to continue to monitor for a slip of the other hip.
Complications
-
Typically seen only in unstable slips, avascular necrosis is one of the most common complications of SCFE. In some cases, the slippage of the femoral head can cause blood supply to the bone to become limited.
This can trigger the collapse of the femoral head and its surrounding cartilage, ultimately leading to painful arthritis in the hip. In some cases, further hip reconstruction surgery may be necessary.
-
Chondrolysis involves a rapid degradation of the articular cartilage in the hip, leading to severe pain and reduced range of motion in the hip joint. While the cause is not fully understood, it is hypothesized that it may result from inflammation in the hip and its surrounding tissues.
In order to restore range of motion, patients typically receive anti-inflammatory medications and aggressive physiotherapy.
-
Some SCFE patients may develop a limb length discrepancy due to avascular necrosis or growth arrest in patients who are treated with in-situ fixation.